Adolf Meyer and the myth/reality of mental illness:
implications for current understanding
D. B. Double
Norfolk Mental Health Care NHS Trust &
School of Health Policy and Practice, University of East Anglia
The model of mental illness adopted by the psychobiology of Adolf Meyer is compared to that of biomedical psychiatry. Mainstream psychiatry's attack on anti-psychiatry for its denial of the reality of mental illness has obscured the extent to which some so-called anti-psychiatrists, such as R. D. Laing, adopted a biopsychological model of mental illness, not dissimilar to the approach of Adolf Meyer. The strength of a biopsychological understanding of mental illness should not be underestimated in present-day psychiatry.
The monograph entitled The reality of mental illness (Roth & Kroll, 1986) represents the culmination of traditional psychiatry's response to what has been called 'anti-psychiatry'. Anti-psychiatry, exemplified by psychiatrists such as R. D. Laing and Thomas Szasz, is commonly perceived as a passing phase in the history of psychiatry (Tantum, 1991). From this perspective, the book by Roth and Kroll is seen as providing the final 'death-blow' to the intellectual argument of anti-psychiatry.
Historical distance is permitting a more positive assessment of the contribution of 'anti-psychiatry'. For example, Cultures of Psychiatry and Mental Health Care in Postwar Britain and the Netherlands (Gijswijt-Hofstra & Porter, 1998) contains papers given at a workshop held in June 1997 in Amsterdam organised by the Wellcome Institute for the History of Medicine (London) and the Dutch Huizinga Institute for Cultural History. It puts the views of anti-psychiatry in their broader cultural context and sees their continuities rather than discontinuities with the present state of psychiatry. Similarly, the Philosophy Special Interest Group of the Royal College of Psychiatrists has recently held its second annual R. D. Laing conference. This coincides with a steady stream of biographies which have recently been published about Laing now more than 10 years after his death and more than 30 years after his rise to fame with the "counter-culture" of the 1960s (eg. Burston, 1996, Kotowicz, 1997, Laing, 1994, Mullan, 1999). This demonstrates at least an interest in what Laing personified in psychiatry and encourages a re-examination of his ideas.
Roth & Kroll (1986) also survey their own position in historical perspective. They see the 1950s as dominated by post-Freudian views with biological psychiatrists in a minority. The 'flirtation with the view that mental illnesses have primarily psychological causes' (p.75) is regarded in retrospect as a brief interlude in the history of psychiatry, covering no more than the period 1900-1970. During the 1960s and certainly by 1970 in the USA, the biological model of mental illness is seen as having reasserted its dominance, as the power and attractiveness of Freudian psychology declined.
There may be a debate about whether psychological approaches have ever reached an ascendancy in psychiatry (Clark, 1981). Somatic explanations of mental illness have probably always dominated psychiatry and there has been a corresponding tendency to disparage psychological alternatives. Nonetheless, the period 1900-1970 did see the development and influential era of psychoanalysis. The first half of the century also saw the formulation of Psychobiology, a term used for the work of Adolf Meyer (1951/2). He had an important role in American psychiatry and his ideas came to Britain via psychiatrists such as David Henderson and Aubrey Lewis (Gelder 1991).
In this paper I want to concentrate on Meyer's notion of mental illness and contrast it with the biomedical model of mental illness, using Roth and Kroll as representatives of the biomedical view. I want to relate these understandings about the nature of mental illness to ideas in "anti-psychiatry", particularly by R. D. Laing. I then want to discuss the implications of a Meyer's biopsychological model of mental illness for the current state of psychiatry.
Comparison of the idea of mental illness in Meyerian and biomedical psychiatry
Meyer (1951/2) and biomedical psychiatry find different ways of accommodating to two main philosophical issues (i) the mind-body problem and (ii) the application of scientific method to the study of human nature.
(i) The mind-body problem.
Meyer (1951/2) had a very broad notion of the 'body', seeing biology as to do with being human. He wanted to avoid a dualistic solution or the 'doctrine of psychophysical parallelism', as he called it. He argued for mind-brain integration, bringing the mind and body together in his concept of psychobiology. The implication was that 'the person' was seen as the essential setting for psychiatric and indeed all medical practice. Although he maintained an interest in neuropathology, biological considerations hardly ever arose in dealing with everyday psychiatric problems.
Roth & Kroll (1986) say that they too want to avoid a reductionist solution. To quote from them: 'We are not advocating a reductionist position with regard to the relationship between neural events and mental events. ... Reductionism would equate the two. Yet we cannot ignore the brain state underlying ... behaviour.' (p. 76) The implication is that biological abnormalities are the cause of mental illness. This is particularly the case with presentations of mental illness which are outside the normal range of human experience. These correspond to experiences which Karl Jaspers (1963) identified as "un-understandable". Jaspers used this conception as his definition of psychosis.
In contrast, Meyer (1951/2) favoured a psychogenic explanation of mental illness and regarded mental illness as not so completely foreign to normal experience. In particular, disagreeing with Kraepelin, he contended that dementia praecox (schizophrenia) was a maladaptation that could be understood in terms of the patient's life experiences . He found 'in many a case of dementia praecox far more forerunners of actual mischief than the average alienist gets at by his examination when he avoids the facts or does not know how to use them' (vol. II, p. 583). Meyer was opposed to the idea that a hypothetical underlying lesion should be postulated just because some mental disorders may seen unintelligible.
Instead, Roth & Kroll (1986) speculate that abnormalities at a biochemical level, such as neurotransmitters and receptor sites 'will be discovered in some schizophrenics, but perhaps not all' (p. 70). They believe that biological approaches promise to provide certain answers in the future, 'just as the discovery of a spirochaete as the aetiological agent in syphilis provided certain answers at the turn of the [last] century' (p. 70). The science of psychiatry has moved on since Roth and Kroll wrote these words to an emphasis on studies of brain neuroimaging rather than psychopharmacological studies of neurotransmitters. The dominant hypothesis of schizophrenia is now the neurodevelopmental hypothesis (Andreassen, 1999). Underlying this hypothesis is still the notion that abnormalities of neural connectivity are the cause of mental illness.
Roth & Kroll (1986) recognise that the biological position is a hypothesis. Nonetheless, they suggest that 'a disease hypothesis seems as justified as any other formulation' (p. 9). They also acknowledge the potential for overgeneralization in such a hypothesis. Although the biological hypothesis may be a dominant hypothesis, they accede that 'it does not wholly invalidate alternative hypotheses' (p. 4).
In contrast, Meyer (1951/2) recognised the danger in focusing too much on the brain, avoiding understanding the patient as a person. He was fond of calling a 'neurologising tautology' any attempt to reduce accounts of personal problems to brain diseases.
It is difficult to reconcile these two perspectives on mental illness, which at least potentially have very different consequences for its management.
(ii) The importance of the scientific method.
Meyer (1951/2) had a broad notion of science which included the study of the person. He took over the Huxleyan notion of science as being 'organised commonsense'. He hoped that the viewpoint that science could only have a physical basis and therefore not be applied to mental life 'would become archaic' (vol. II, p. 573).
In contrast, Roth and Kroll's view of science is positivist. They do not explicitly mention Meyer in their book. Instead they refer to the biopsychosocial model of Engel (1977), which will serve as an adequate substitute for the purposes of this paper. Roth and Kroll criticise Engel's model as vague. In the Mayer-Gross textbook of which Roth was co-editor with Slater, the Meyerian approach is described as "almost entirely sterile" (Slater & Roth, 1969). To quote from Roth & Kroll (1986) - 'Such a closure of the model at the level of vague statements that all factors are important and must be taken into account threatens to interfere seriously with the continued progress of medicine' (p. 64).
Both Meyer (1951/2) and Roth & Kroll (1986) agree that the definition of mental illness is a functional not structural definition. Mental illness indicates abnormal mental functioning. They diverge on the value of diagnosis and classification for psychiatric practice. For Meyer, the 'facts of the case' are details about the person. The first aim of the psychiatrist should be to get at the 'facts of the case' rather than to make a diagnosis, and making a diagnosis may not even be possible. Roth and Kroll see more advantage in making an analogy between mental and physical illness. To quote from them, 'We have a diagnostic system that divides diseases into discrete categories because we find it easier to think and work this way, ...' (p. 77) They also acknowledge the ways in which mental illness is not like physical illness, suggesting that a diagnostic system does not necessarily provide a 'more 'accurate' representation of how things are in nature' (p.77).
Meyer was fond of seeing the psychobiological point of view as an advance over the organic views of the past. Roth and Kroll counter by saying: '[P]recise knowledge is lacking and it does not serve the cause of the biopsychosocial model to put it forward as a doctrinal truth which resolves the major problems of clinical practice' (p. 66)
It may be true that the philosophical basis of Meyer's Psychobiology is more rigorous than the biopsychosocial model of Engel which is the actual target of Roth and Kroll's remarks. Nonetheless, there is a perceived certainty about the biological viewpoint, which is highly valued and gives an apparent justification to the hypothesis. As there are difficulties in deciding a priori between the legitimacy of the biomedical and biopsychological models of mental illness, factors like this do sway heavily.
Models of mental illness in anti-psychiatry
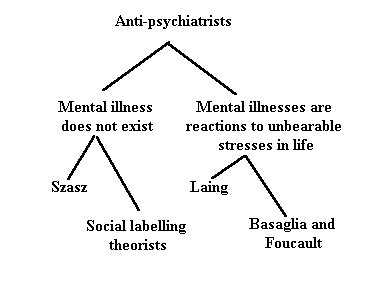
It is necessary to recognise that anti-psychiatry is not a homogeneous set of views. There are at least four separate groupings (see figure).
Figure
The main dividing line is between those that argue that there is no such thing as mental illness, and those that say that mental illnesses are not diseases in the medical sense, but are reactions to unbearable stresses in life. The first group can be further subdivided into those that state that mental illness does not exist in a primary sense, or in the words of Thomas Szasz (1972), who is the main proponent of this group, that 'mental illness is a myth'. The other subdivision would be those identified as social labelling theorists (eg. Scheff, 1966) who suggest that mental illness does not exist in the sense that it is merely the secondary consequence of identification by others in society.
The group who recognise that the use of the term mental illness is metaphorical and do not want to minimise the suffering of people with mental health problems can also be subdivided into two. The first would contain Laing (1967), who emphasises that reactions identified as mental illness relate to interpersonal behaviour, particularly within the family. The second subdivision, containing authors like Basaglia (Scheper-Hughes & Lovell, 1987) and Foucault (1971), emphasise the broader societal factors involved in presentations of mental illness.
The anti-psychiatrists that go as far as saying that mental illness does not exist are easy prey for the arguments of Roth and Kroll. Thus, for example, Szasz is attacked for holding a 'dualistic viewpoint' (p. 55). Szsaz's view that 'to talk of mental disease is to commit a category error' leads logically to his opposition to involuntary hospitalisation and the insanity defence. However libertarian these views may be, they do not necessarily make society more humane.
Similarly, the social labelling theorists are dismissed because of their lack of evidence for the claim that "primary deviance" falls within a normal frame of mind and is of minor consequence. Although Roth & Kroll (1986) accept that institutionalisation can increase the symptoms of schizophrenia, they do not concede that social labelling by professionals in the form of diagnosis and treatment can be its origins.
Roth and Kroll's rebuttal of anti-psychiatry is less forcefully directed at Laing, Basaglia and Foucault. These authors are included in the overall sweep of their denunciation, although their differences from Szasz and the social labelling theorists are acknowledged. In particular, Laing and Foucault are dismissed as romantics derided for apparently having Rousseau as an 'intellectual godfather' and for being too affected by the idea of the 'noble savage'. Recognition of the personal alienation caused by society is said to subjective, emotional and to lead to substitution of fact for allegory.
Implications for a biopsychological model of mental illness
However correct Roth and Kroll's characterisation of Laing may be, I want to concentrate on Laing's model of mental illness. The main point is that he had essentially the same model as Adolf Meyer. The two main groups of anti-psychiatrists are lumped together in criticism by Roth and Kroll. It therefore goes unrecognised how close one of these groups is to the mainstream psychiatry of Adolf Meyer. In their marginalisation of the anti-psychiatrists, Roth and Kroll substitute their biological model and thereby undermine the biopsychological approach of Meyer.
As far as I know, Laing was not directly aware of the work of Adolf Meyer. He does acknowledge the influence of similar ideas, such as the interpersonal psychiatry of Harry Stack Sullivan (1953). He also recognised the significance of the William Alanson White Foundation, where there was a tradition of analogous views, albeit modified from psychoanalysis (Mullan, 1995).
Laing and Meyer could be said to have had a similar ambivalent relationship to psychotherapy. Meyer's Psychobiology was distinct from psychoanalysis, although he was open to psychotherapeutic ideas (Leys, 1981). The professional division of biological psychiatry from psychotherapy is readily recognised, concealing how much Meyerian Psychobiology provides a 'third way' in psychiatry. Meyer's social perspective goes beyond the voluntary individual practice of psychotherapy.
Laing of course never went back to mainstream psychiatry after Kingsley Hall (Mullan, 1999). At times he tried to maintain links with the psychiatric profession and sought its endorsement. Part of the reason why he could not go back was that his training had left him stranded in the framework of individual psychotherapy. He found it difficult to practice humanely from his perspective within traditional psychiatric practice, as others have done who adopt his viewpoint.
The Politics of Experience (Laing, 1967) is commonly regarded as the more radical version of Laing's views, taking him beyond the pale of mainstream psychiatry to which he is regarded as having made a significant contribution with earlier books like The Divided Self (Laing, 1964). This argument may well have been overstated and the continuity in development of Laing's thinking needs to be acknowledged (Mullan, 1999). So that no-one can doubt that I am quoting from the works of Laing that are regarded as 'authentic anti-psychiatry', the following quotes are all taken from the Politics of Experience (Laing, 1967). Laing himself, of course, always disavowed the term anti-psychiatry.
Both Laing and Meyer recognised that the term mental illness is used metaphorically. To quote from the Politics of Experience: 'There is no such 'condition' as 'schizophrenia', but the label is a social fact and the social fact a political event' (p. 100) Similar sounding radical statements can be found in Meyer (1951/2): for example, 'Very often the supposed disease back of it all is a myth and merely a self-protective term for an insufficient knowledge of the conditions of reaction' (vol. II, p. 585). In this quote there are even echoes of Szasz's use of the term 'myth' of mental illness.
Furthermore, both Laing and Meyer recognise the psychological aetiology of mental illness. To quote from Laing (1967): '[I]t seems to us that without exception the experience and behaviour that gets labelled schizophrenic is a special strategy that a person invents in order to live in an unlivable situation' (p. 95). For Meyer, patients become mentally ill 'by actually living in ways which put their mind and the entire organism and its activity in jeopardy' (vol. IV, p. 4).
Both Laing and Meyer do not take a deterministic view of the science of human nature. Laing is commonly criticised for apparently suggesting that the family, particularly the parents, are the cause of schizophrenia (Clare, 1997). This criticism is invalid. To quote from the Politics of Experience: ' ...[It is not] a matter of laying blame at anyone's door. The untenable position, the 'can't win' double-bind, the situation of checkmate, is by definition not obvious to the protagonists' (p. 95). Laing took an interest in Sartre's concept of dialectical rationality and translated Sartre's work with David Cooper in the book Reason and Violence (Laing & Cooper, 1964). He would not have been so naive as to suggest that what he was proposing was a causal one-to-one connection between schizophrenia and the family. The unfortunate fact is that such misinterpretations of Laing have discouraged further study of the family context of mental illness.
Similarly, Meyer's understanding of a science of persons was not a reductive causal analysis but an emphasis on the understanding of human action. He knew that his approach would be 'scoffed at because it looked as if one was not dealing with dependable and effective data' (vol. IV, p. 4). Nonetheless he thought it important for a psychiatrist to grapple with 'the relativity of all the factors with which he has to deal in our field' (vol. III, p. 31).
Both Meyer and Laing thought that it was a mistake to go beyond the step of realising that the biological hypothesis is a hypothesis to acting on the hypothesis in practice. To quote from Laing (1967): '... [I]t is wrong to impute to someone a hypothetical disease of unknown aetiology and undiscovered pathology unless ... [it can be proved] otherwise' (p. 87). Similarly, Meyer (1951/2) understood the 'craving for logical unity' in the diagnosis and classification of mental illness but did not think that this justified giving a false impression that matters were known or 'sufficiently settled for practical purposes' (vol. II, p.136).
I do not want to cloud the comparison of Laing and Meyer by mentioning in detail Laing's so-called transcendental or psychedelic hypothesis of mental illness (Siegler et al, 1972). Laing himself complained that too much was made of his comments about schizophrenia being a "voyage" and a natural healing process (Mullan, 1995). This apparently positive valorisation of schizophrenia has been used to disparage his position in psychiatry (Clare, 1997). Yet Laing did not fail to recognise the suffering of people diagnosed as schizophrenic. He also accepted later in life that Kingsley Hall was only a partial success (Mullan, 1995). Several other psychoanalytic writers besides Laing, such as Harold Searles, have written about the defensive value of psychosis (Kotowicz, 1997). Laing's ideas should not be dismissed because of his excesses. In particular it is important to recognise that his fundamental model of mental illness was biopsychological like Adolf Meyer.
Conclusion
The dominant tradition of mental illness in psychiatry is of the biomedical model. Although Meyer attained an influential position within institutional psychiatry, Laing was marginalised as an "anti-psychiatrist". Laing's ideas were associated in "anti-psychiatry" with others like Szasz who deny the reality of mental illness. This mélange of ideas identified as "anti-psychiatry" was marginalised in the hegemony of biomedical psychiatry.
A conceptual distinction needs to be made between the models of mental illness of Ssasz and Laing. This then allows the congruence of the models of Laing and Meyer to be acknowledged. The value of biopsychological ideas like those of Laing and Meyer needs to be reinforced. Their strength in the current state of psychiatry should not be underestimated.
References
Andreassen, N. (1999). Understanding the causes of schizophrenia. New England Journal of Medicine, 340, 645
Burston, D. (1996). The wing of madness. Cambridge, Mass: Harvard University Press
Clare, A. (1997). In B Mullan (ed) R. D. Laing. Creative destroyer. London: Cassell
Clark, M. J. (1981). The rejection of psychological approaches to mental disorder in late nineteenth century British psychiatry. In A. Scull (ed) Madhouses, mad-doctors and madmen. London: Althone Press
Engel, G. E. (1977). The need for a new medical model: A challenge for biomedicine. Science, 196, 129-36
Foucault, M. (1971). Madness and civilisation. London: Tavistock
Gelder, M (1991). Adolf Meyer and his influence on British psychiatry. In G.E. Berrios & H. Freeman, (eds), 150 Years of British Psychiatry, 1841-1991. London: Gaskell
Gijswijt-Hofstra, M. & Porter, R. (eds) (1998) Cultures of psychiatry and mental health care in post-war Britain and Netherlands. Amsterdam: Clio Medica
Jaspers, K (1963). General Psychopathology. (Trans J. Hoenig & M. W. Hamilton). Manchester: Manchester University Press
Kotowicz, Z. (1997) R.D. Laing and the paths of anti-psychiatry. London: Routledge
Laing, A. (1994) R.D. Laing. A biography. London: Peter Owen Publishers
Laing, R. D. (1964). The divided self. Harmondsworth: Penguin
Laing, R. D. (1967). The politics of experience and The bird of paradise. London: Penguin
Laing, R. D. & Cooper, D. G. (1964) Reason and violence. London: Tavistock Publications.
Leys, R. (1981). Meyer's dealings with Jones: A chapter in the history of the american response to psychoanalysis. Journal of the History of Behavioural Sciences, 17, 445-465
Meyer, A. (1951 & 1952) Collected Papers (Four Volumes) (Ed. E. Winters). Baltimore: John Hopkins University Press.
Mullan, B. (1995) Mad to be normal. London: Free Association Books
Mullan, B (1999). R.D. Laing. A personal view. London: Duckworth
Roth, M & Kroll, J. (1986). The reality of mental illness. Cambridge: Cambridge University Press
Scheff, T. (1966). Being mentally ill. Chicago: Aldine
Scheper-Hughes, N. & Lovell A. M. (1987) Psychiatry inside out: Selected writings of Franco Basaglia. New York: Columbia University Press
Siegler, M., Osmond, H., & Mann, H. (1972) Laing's models of madness. In R. Boyers & R. Orrill (eds). Laing and anti-psychiatry. Harmondsworth: Penguin
Slater, E. & Roth, M. (1969) Clinical psychiatry. (Third edition). London: Bailliere, Tindall & Cassell
Sullivan, H. S. (1953) Conceptions of modern psychiatry. New York: Norton
Szasz, T. S. (1972). The myth of mental illness. London: Paladin
Tantum, D. (1991). The anti-psychiatry movement. In G.E. Berrios & H. Freeman, (eds), 150 Years of British Psychiatry, 1841-1991. London: Gaskell