MADNESS, MURDER & MEDIA
A Realistic Critique of the Psychiatric Disciplines in Post-liberal Society
Dr Peter Morrall
Senior Lecturer in Health & Sociology
University of Leeds, UK
April 2002
INTRODUCTION
On Saturday 3rd June 2000, the Guardian newspaper, a stalwart of politically correct thought and liberal-left opinion, ran three separate stories about violence committed by mentally disordered people. The first story referred to a Greek female 'axe murderer' who was being released from a prison psychiatric ward. Next was the account of a British male 'sword attacker', reported as suffering from paranoid schizophrenia, who had injured eleven people attending a church service. Third, was coverage of a Tunisian man, described as being a 'violent loner with a long history of mental illness', who took hostage dozens of children at gunpoint in Luxembourg.
Ostensibly, this journalistic 'overkill' about the danger posed by the mad seems to confirm conventional wisdom within the mental health industry regarding media portrayal of an already socially tarnished group:
...our view is that the media are highlighting a tiny minority of cases relative to the very large number of people with mental health problems, and that in doing so media accounts are distorting public perceptions of the whole area of mental health.
(Philo, 1996, p.xii)
There are many misconceptions about psychiatric patients. Surveys consistently show that the general public believe they are unpredictable, potentially dangerous, and likely to commit violent and sexual crimes…..This damaging and inaccurate picture is heavily reinforced by the media, where headlines like ‘Ex-mental patient sought by police’ and Mad axeman kills two’ are never balanced by more positive reports (‘Ex-mental patient elected mayor’ or ‘Former patient rescues drowning girl’).
(Johnstone, 1989, p.21).
Indeed, it has become platitudinous to acknowledge that only a small number of psychologically disturbed people are a danger to others. Individuals diagnosed as schizophrenic are much more likely to commit suicide than murder. The number of homicides carried-out by 'normal' people is growing, whereas the homicide rate amongst the mentally disordered is relatively static (Appleby, 1999; Taylor and Gunn, 1999).
Moreover, it is a truism that diagnostic certainty surrounding mental disorder is elusive, and that the boundaries between 'madness' and 'badness' are difficult to delineate. For example, can such a distinction be made between the killing of four generations from one family in an arson attack carried-out by Richard Fielding (for which he was found to have 'diminished responsibility'), and the killing of fifteen women patients by Dr. Harold Shipman (for which he was given 15 life sentences)? How was it that a court in Texas found Andrea Yates, with a history of postpartum psychotic depression and attempted suicide, guilty of capital murder for drowning her children?
I argue here that the media is not simply engaging in yet another a 'moral panic' by highlighting ‘mad murders’, but reflecting justifiable anxiety about the perceived danger from mentally disordered people in the community and the apparent ineptitude of mental health services and personnel.
Furthermore, I suggest that the psychiatric disciplines (specifically medicine and nursing) have contributed to a period of unprecedented public and media alarm about the risk from mentally disordered people by disowning the problem. As a consequence, post-liberal social control (‘hyper-control’) over mentally disordered people has been further legitimised.
THE STUDY
Data are presented in Madness and Murder from a five-year study (1994-1999) of media representations of homicides and non-fatal violence conducted by people described as mentally disturbed. Data continue to be collected post-1999.
Approximately two thousand British newspapers (hard copy), and over one thousand 'electronic' articles, were scrutinised. The content of these articles was contrasted with the 'facts' furnished by reports of independent inquiries into murders involving the mentally disordered. Most of the incidents occurred in Britain. Eight, however, were committed outside of Britain (one each in the West Indies, Israel, and Germany, and five in the USA). Three of those committed in other countries, however, involved British citizens (as victims).
There were ninety-four incidents reported in the newspapers during the period of the study, involving one hundred and sixteen killings (i.e. some of the incidents involved more than one death). Eight of the killers committed suicide.
The most common method of killing was caused through stabbing or slashing the victim (n = 44: 38%). Fourteen (12%) victims were bludgeoned to death with a blunt instrument such as a hammer. Ten (8.6%) people were strangled or suffocated. Eleven (9.5%) died as a result of being shot, six (5.2%) were burnt to death, five (4.3%) poisoned, two (1.7%) dropped from a height, and two (1.7%) blown-up by a grenade. No mention was made of how twenty-two (19%) of the victims met their deaths.
Forty-four (47%) of the ninety-four killers had a primary diagnosis of psychosis (principally schizophrenia), and eighteen (19%) of personality disorder (including Muchausen's syndrome, and alcoholism). Nine (9.6%) of the killers were described as suffering from depression. A dual diagnosis was attached to seven (7.4%) of the killers, but for sixteen (17%) no specific diagnosis was given.
The vast majority of the killers were men (n = 78: 83%). The gender of the victim was not mentioned in thirty-two (27.6%) of the cases. Where the gender was identified, however, more women had been killed (n = 45: 38.8%) than men (n = 39: 33.6%).
Fifty (43%) of those who died were unknown to the killer, whilst thirty-eight (32.8%) were closely related (present or former spouse/lover, parent, child, or sibling of the killer). The number who died who were associates of the killer (neighbours; friends; fellow patients in psychiatric care or prison 'cell-mates') was twenty-four (20.7%). Four (3.4.%) mental health workers were also killed.
The court verdicts in the British cases (where known, and other than when the suspect committed suicide) were: manslaughter with diminished responsibility (44 -two of whom were also found guilty of attempted murder); manslaughter (2); murder (11 - three of whom were also found guilty of other serious offences); unfit to plead (2); not guilty by reason of insanity (7); infanticide ( 1). The majority (39) were sent to high security hospitals indefinitely.
DISCUSSION
Compared to a list that could have been compiled of all murders committed over the five years of this study, the inventory of murder and mutilation by the mad may not be considered by senior representatives of the psychiatric disciplines to be significant. However, the summation of people affected directly or indirectly by mentally disturbed killers alone runs into thousands, if not millions.
In each instance there is the wasted life of the victim, and the dramatically altered life-course of the culprit. The lives of close family members and friends of each will be displaced to a devastating extent in the short-term and quite possibly permanently. Added to this computation of distress is the re-shaping, either moderately or severely, of the lives of the victim's and culprit's associates (for example, neighbours, colleagues, and other relatives).
Furthermore, rumour mongering and media reporting causes the anguish to ripple through the wider population. In this sense, as with all murders, it is the 'community' that has been violated.
However, unlike 'normal' killings, murders by the mentally disordered are not only perceived to undermine the safety of the citizen, but also the 'rational' basis of the social system. It is the 'madness' of the individual murder, not the absolute or relative number of murders by the mad, that generates psychological and social instability. Warranted or not, the unpredictability and incoherence of the mentally disordered killer disturbs both the ontological security of the individual citizen and the normative imputations of the conscience collective. Consequently, the killing by those deemed to be mentally disordered is a public issue beyond that of other forms of crime.
The newspapers (tabloid and broadsheet) are guilty of sloppy, careless and injudicious journalism in the reporting of mad-murders. Pejorative expressions spatter the narrative and captions of stories covering violent and homicidal incidents involving the mentally disordered:
BRAZIL NUTTER: Ronaldo had mental breakdown night before France [world cup football] final.
(Daily Mirror, 14th July)
HE'S A RAVING NUTTER: World exclusive on Mental patient who stole a kiss from [the late Princess] Di.
(Daily Star, 9th November)
A PSYCHOTIC ON THE LOOSE IN SUFFOLK
(The Guardian, 18th February, 1999 – ironical reference to Benjamin Britten's play 'Peter Grimes')
The media can also be accused of exaggerating the culpability of the professionals who had prior dealings with the murderer, and thereby colluding in the ‘institutional sacrifice’ of individual employees, allowing NHS management and governments to avoid the responsibility for inadequate service provision. However, the newspapers are reproducing evidence from independent inquiries which invariably point to both people and system failures:
The Guardian
Wednesday November 28 2001
NATIONAL NEWS
Hospital errors freed man who killed two
Tania Branigan
A paranoid schizophrenic man known to have access to guns killed two people and injured three more after a catalogue of errors by nursing and medical staff led to his release from hospital [in 1996], an independent report stated yesterday….. Kieran Coonan QC, chairman of the inquiry panel, described Hutchinson’s treatment by the hospital as "very, very, very poor indeed". But he added: One cannot ignore the difficulties and the fundamental lack of resources". Discussing the damning report, the medical director of the South London and Maudsley NHS Trust, which now covers the area [of the hospital in the report], said "…..Clinical teams are [still] making difficult decisions, discharging patients who perhaps in an ideal world they’d keep inside".
But a proportion of the blame for media amplification and public panic rests with the psychiatric disciplines for not acknowledging the gravity of ‘madness and murder’ and thereby not offering the public appropriate reassurance. Long-term damage has been done to community acceptance of the mentally disordered because of the inadequate and sometimes antagonistic response by the psychiatric disciplines to genuine and understandable (if inflated) fears about the risk posed by this group. Moreover, the response of the State, in the face of professional ‘irresponsibility’, has been to justify and increase post-liberal policies and laws that further confine and de-emancipate mentally disordered people.
POST-LIBERAL SOCIAL CONTROL
In mature liberal-democracies there has been a major shift in social control measures as a consequence of the fashioning of a new social contract of rights and responsibilities. The denizen becomes citizen. He/she is expected by the State to be, and he/she demands of himself/herself, unprecedented (in modern times) involvement in decision-making within many (if not all) spheres of civil life. He/she is given the privilege of social inclusion, and has an ethical obligation to participate in the operation of social affairs at the local and national level. No longer will the principles of the free market (no social responsibility, only self-responsibility) or socialism (no self-responsibility, only social responsibility) be the only available political ideologies. This is what Anthony Giddens (2000) describes as the ‘Third Way’.
As Nikolas Rose (2000) has suggested, under such socio-political conditions, with an expanding and demanding citizenship, the system of social control has to accommodate and vitalize the active and 'free' subject (through the reward of - apparent - greater freedoms) and denigrate far more robustly (through - very real - harsh punishment) the deviant. Social control in post-liberal society is sophisticated and ubiquitous. It develops as an interwoven pattern of direct and indirect, clandestine and flagrant interventions in daily life – both progressively tolerant (human rights acts; consumer privileges) and at the same retrogressively despotic (diminution or removal of human rights from some sections of society).
In an epoch where self-regulation is key to social control, those that are perceived (by the State and its semi-detached but synergetic agencies) as failed citizens, spoiled citizens, rebellious citizens, or in an underclass of non-citizenship, pose an unparalleled threat to civil constancy. They become susceptible to the concomitant discourse of risk thinking, risk management, and the technologies of risk assessment and control. Defaulting on the responsibilities of the new social contract invites literal or virtual social confinement. Paedophiles, recidivists (adult criminals, young offenders, prostitutes, drunks, noisy neighbours), the severely mentally ill and psychopaths – the ‘dangerous classes’ - are demonised and socially and perhaps physically excluded.
In the UK a plethora of laws and polices has been implemented or proposed to deal with these defaulting groups. From the 1950s onwards policies of de-institutionalised care, and legislation aimed at treating most mentally disordered people as informal patients, were initiated in many parts of the liberal-democratic world. Such liberalism has been reflected in the criminal justice system with, for example, a whole raft of 'community' punishments being used as alternatives to prison, and a system of 'warnings' available for police officers to use where minor offences have occurred.
However, by the late 1990s the UK government rescinded its commitment to libertarianism in these spheres, and incorporated within its political programme a patently coercive agendum.
Within the criminal justice sphere, the following are indicative of this shift:
(a) Mandatory life-sentences for second serious violent or sexual offences (for example: attempted murder; soliciting murder; rape; intercourse with a girl under thirteen years of age; grievous bodily harm; possession of a firearm with intent to injure; possession of a real or imitation firearm during a robbery);
(b) Police registers of Sex Offenders (anyone convicted of a serious sex offence – particularly against children – must submit name and current address to the local police);
(c) Electronic monitoring ('tagging'), ‘voice verification’ call systems, home detention orders, and night-time curfews, for adults and young offenders serving community sentences or release on licence;
(d) Electronic monitoring of young offenders on bail;
(e) Anti-social behaviour orders aimed at, for example, juveniles (over 10 years of age) causing harassment, alarm, or distress, prostitutes, and disruptive neighbours - juveniles have been barred from specified localities for up-to ten years;
(f) Neighbourhood wardens employed to patrol public spaces with powers to enforce fines for dog-fouling, littering, and other forms of anti-social behaviour;
(g) Community payback reparation orders whereby vandals are forced to repair damage they have caused
(h) The compulsory drug testing of offenders and suspects;
(i) Immediate fines for loutish and drunken behaviour on the streets.
(j) A higher profile for victims of crime in sentencing and release;
(k) (Proposed) Indefinite retention of all DNA and fingerprint samples from all suspects.
With regard to the mentally disordered, these following developments have run parallel to those in criminal justice:
(a) The extension of supervision registers for most/all severely mentally ill people living in the community;
(b) (Proposed) Compulsory detention of people with personality disorder without trial and without a crime having been committed;
(c) (Proposed) The re-calling to the psychiatric institution of severely mentally ill people living in the community for compulsory treatment;
(d) The development of the 'electronic panoptican' (i.e. microphone and video surveillance within psychiatric institutions)
(e) The extensive appliance of 'assertive outreach' whereby the 'social space' between the psychiatric institution and the community is supervised;
However, the social control mechanisms listed above mark not so much a shift within liberalism but a crucial and indelible transformation in the social relations between the (non)citizen and the State. We have entered the epoch of 'post-liberalism' (Morrall, 2000).
Moreover, the bombing of the World Trade Center in New York on September 11th 2001 has augmented significantly post-liberalism. In the United States and other Western countries, such as the UK, emergency legislation has resulted in long-term or indefinite detention without trial or criminal charges for suspected terrorists (Norton-Taylor, 2002).
Post-liberalism is not a synonym for ill-liberalism (i.e. a state of complete absence of liberal laws and policies) or anti-liberalism (a deliberate movement to replace all liberal laws and policies). Post-liberalism describes the point at which advanced democratic societies arrive when growing numbers of people (including, for example, consumers of health services, and victims of crime) demand action over particular tensions in civil life. Post-liberalism does not, therefore, herald the demise of liberalism per se. Paradoxically, there is an increase in democratic participation and petitioning for, and statutes on, human rights. The prefix 'post' as used here denotes a period 'after' or 'following (in this case 'liberalism') but also 'connected to' the original event. Therefore, the use of ‘post’ is similar to that in the term 'post-modern society' whereby not only was the modern epoch a necessary pre-condition for the accession of post-modernism but key elements of modernism (e.g. materialism; commodification; technological advances) remain.
When self-regulation is not apparent, and the regulatory authorities appear ambivalent about their social responsibility to compensate for the absences of self-responsibility, then ‘hyper-control’ is even more likely. Procedures and laws will be produced to ensure that a target deviant group is vilified and harnessed, with the possibility for other more specialised and obliging agents of social control to be instituted. Such has been the case with the mentally disordered and the psychiatric disciplines.
CONCLUSION
……the social responsibility of caring for the mentally ill is an essential function of psychiatry and should not be neglected.
(Double D, 2002, Critical Psychiatry Network)
Patients and society will continue to demand its [psychiatry’s] services and appreciate realistic expectations.
(Double D, 2002, Critical Psychiatry Network)
Contrary to much of the extant literature on the handling of 'madness' by the press, and the stance taken by most mental health professionals, I conclude that homicide (whether by the 'mad' or 'normals'), is a public health issue which should not only be taken seriously, but whose rates have the potential to be checked. Moreover, the perceived dangerousness of the mentally disordered is realistic. The threat to strangers and the families and associates of the mentally disordered should be dealt with responsibly and overtly by the psychiatric disciplines to prevent further persecution, scapegoating, and post-liberal discipline (i.e. ‘hyper-control’). When psychiatrists and nurses refuse to acknowledge their role as agents of social control, or the reality of the danger posed by a limited number of their patients, they fuel public resentment and media panic.
Social Scientists (and renegade psychiatrists) who promote the notion that madness does not exist (what is called madness being viewed as the product of a process of labelling, or the exercise of power), do little to help raise respect for their discipline. To deny that madness is, no matter in what cultural manifestation, an agonising and (usually) unwanted experience, is to be 'unreasonable'. To point out how social exclusion, stigma, bad habitation, and materialism, add to psychological suffering, is a far more realistic contribution to the debate over madness. To enhance the chances of mentally disordered people becoming ‘citizens’ with full human rights it is necessary to accept the reality of madness as well as the reality of the role of the mad professions.
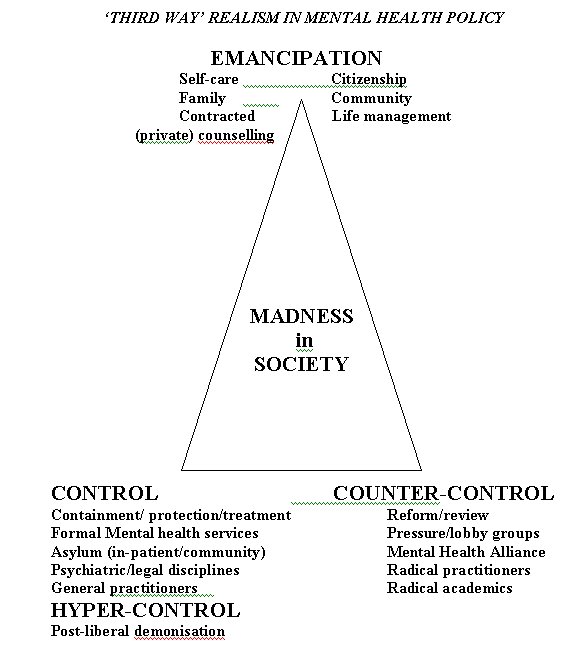
Human psychological emancipation is demonstrable when individuals manage their lives through their own social capital (with or without the assistance of hired helpers), independent of the psychiatric disciplines whether conventional, alternative, or critical (see Appendix 1).
REFERENCES
Appleby L (1999) Safer Services: National Inquiry into Suicide and Homicide by People with Mental Illness. London: Department of Health.
Double D (2002) Critical Psychiatry. Critical Psychiatry Network Website http://www.uea.ac.uk/~wp276/psychiatryanti.htm.
Giddens A (2000) The Third Way and its Critics. Cambridge: Polity Press.
Johnstone L (1989) (1st edition) Users and Abusers of Psychiatry. London: Routledge.
Morrall P A (2000) Madness and Murder. London: Whurr.
Norton-Taylor R (2002) Terror crackdown ‘encourages repression’. Human rights responses to September 11. The Guardian, 17 Jan.
Philo G (1996) (editor) Media and Mental Distress. London: Longman.
Rose N (2000) ‘Government and control’. British Journal of Criminology, 40 (2), 321-339.
Taylor P J and Gunn J (1999) ‘Homicides by people with mental illness: myth and reality’. British Journal of Psychiatry, 174, 9-14.
APPENDIX 1